27 year old active female with pain in the elbow since 2 years.
She was treated as golfer’s elbow for 6 months, without relief.
Radiographs


- Well defined, lytic, expansile lesion in the meta epiphysis region of humerus and ulna
- The lesion in the ulna extends up to the subarticular region, the humeral lesion spares the subarticular zone
- Narrow zone of transition
- Sclerotic margins
- Overlying cortical thinning (arrows) but no frank breach
- No matrix mineralization
- No ground glassing
- No periosteal reaction No periarticular soft tissue density
Differentials on radiographs
- Multicentric giant cell tumor
- Fibrous dysplasia
- Low grade chondrosarcoma
MRI

T1
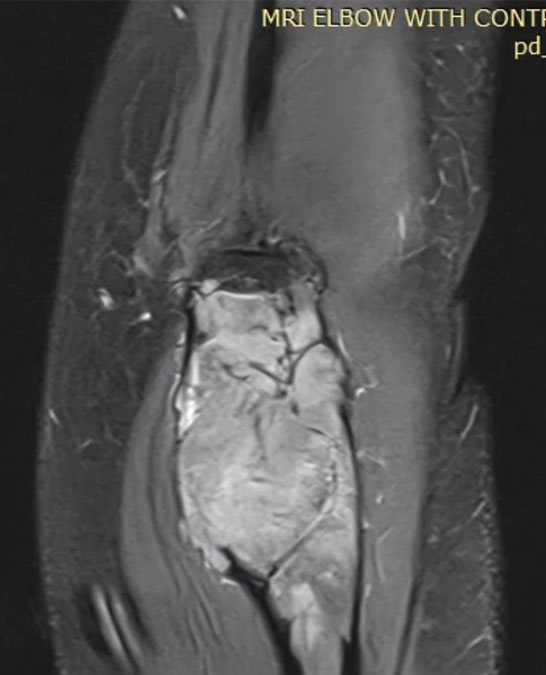
PD
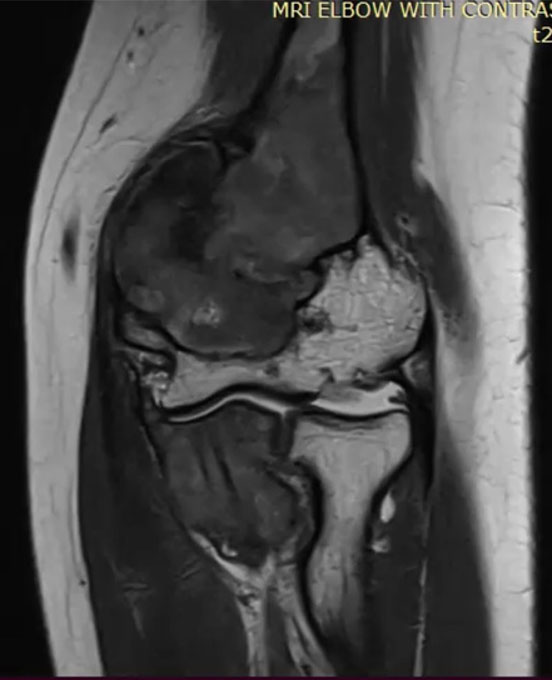
T2
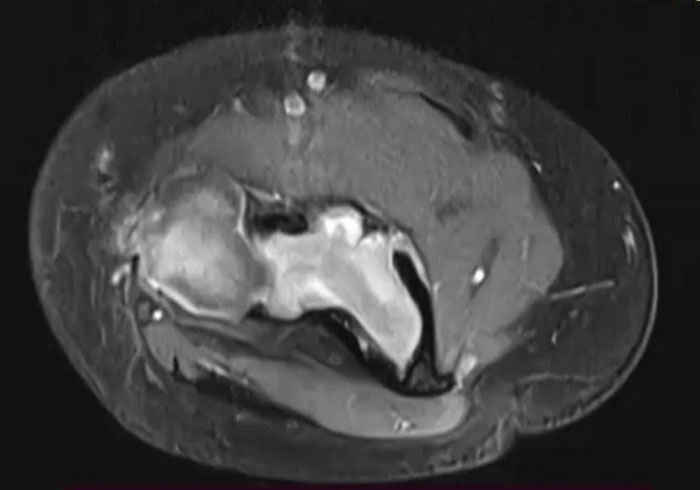
T1 post contrast
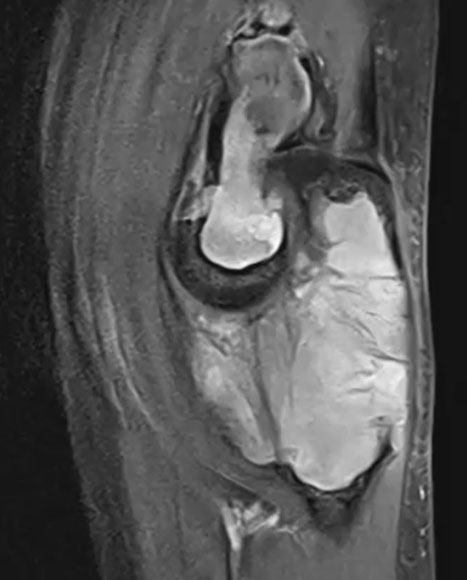
MRI features: Well defined soft tissue, T1 / T2 low signal, areas of cortical breach in distal humerus anteriorly, No blooming on GRE, no perilesonal bone marrow edema, no fluid fluid levels homogeneous post contrast enhancment
MRI differentials narrowed down to:
- Multicentric giant cell tumor
- Fibrous dysplasia
Biopsy was performed because management depended upon diagnosis.
GCT → complete tumor eradication (intralesional curettage + bone cement/ graft or en-bloc resection), denosumab therapy
FD → More conservative approach, follow up, bisphosphonate therapy, cortical bone graft and internal fixation (to prevent pathological fracture).
Biopsy from the left distal humerus and proximal ulna confirms a fibro-osseous lesion consistent with fibrous dysplasia (FD).
Key pathology features:
- Irregular curvilinear trabeculae of woven bone in a fibrous stroma.
- Classic “Chinese character” trabecular pattern.
- No significant osteoblastic rimming.
- No cytologic atypia, mitosis, necrosis, or malignant transformation.
- IHC for H3F3A(H3.3 G34W – molecular mutation seen in 95% of GCT) → NEGATIVE
Involvement of multiple adjacent bones within a single limb segment (distal humerus + proximal ulna) favors: Polyostotic monomelic fibrous dysplasia (polyostotic FD confined to one extremity).
Features
| Feature | Giant Cell Tumor | Clear Cell Chondrosarcoma | Fibrous Dysplasia |
|---|---|---|---|
| Age | Skeletally mature (20–40 yrs) | Adults (20–50 yrs) | Younger patients |
| Location | Eccentric epiphyseal/meta-epiphyseal reaching subarticular bone | Epiphyseal/meta-epiphyseal | Usually metaphyseal/diaphyseal |
| Margin | Well-defined, narrow transition zone | Well-defined, may have sclerotic rim | Well-defined with thick “rind” sclerosis |
| Matrix | Usually no matrix mineralization | Chondroid calcification (rings/arcs) | Ground-glass matrix |
| Expansion | Expansile remodeling common | Mild-moderate expansion | Smooth bony expansion |
| Cortex | Cortical thinning ± breach | Cortical thinning/destruction possible | Cortical thinning with maintained contour |
| Soft tissue mass | May occur in aggressive lesions | Can occur | Rare |
| Key clue | “Soap-bubble” expansile subarticular lytic lesion without sclerosis | Epiphyseal lesion with chondroid calcifications | Ground-glass expansile lesion with rind sclerosis |
Key Points
Multicentric Giant Cell Tumor of Bone:
- Extremely rare → occurs in less than 1% of all GCTB cases. Finding multiple GCT lesions is an exceptional clinical finding.
- While regular GCT affects adults aged 20–40, the multicentric variant targets a significantly younger population (often teenagers and adults around 20 years old) and shows a pronounced female predominance.
- H3F3A(H3.3 G34W – molecular mutation seen in 95% of GCT
Polyostotic FD
- The McCune-Albright Syndrome: Classic clinical triad known as McCune-Albright Syndrome.
- Polyostotic FD
- Café-au-lait skin pigmentation
- Hyperfunctioning Endocrinopathies
- Unilateral Predilection: confine themselves to just one side of the body.
- Somatic Mosaicism: post-zygotic, activating mutations in the GNAS gene.