13 years old female child presented with pain and swelling in the right arm since 3 months

Radiographs
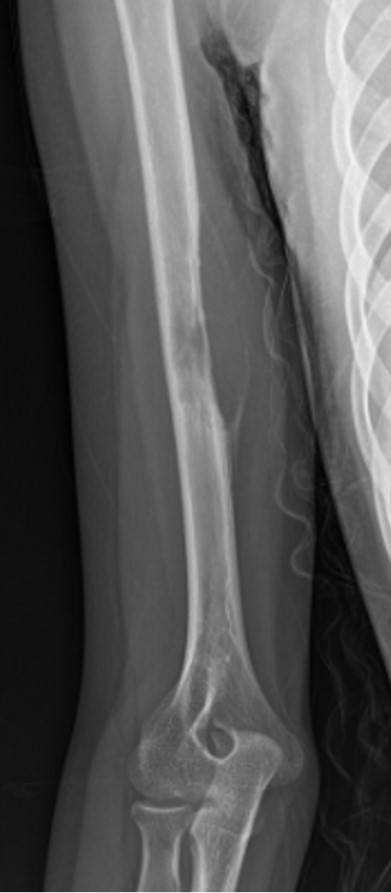
Initial radiographs show eccentric lytic lesion in diaphysis of right humerus with cortical expansion and thinning
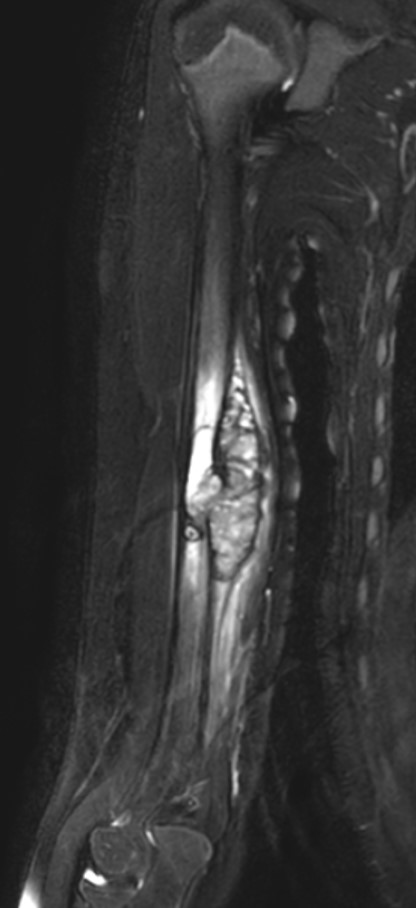
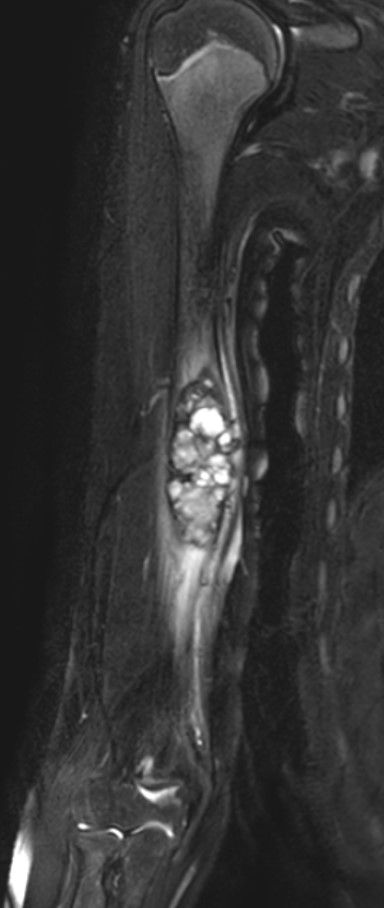
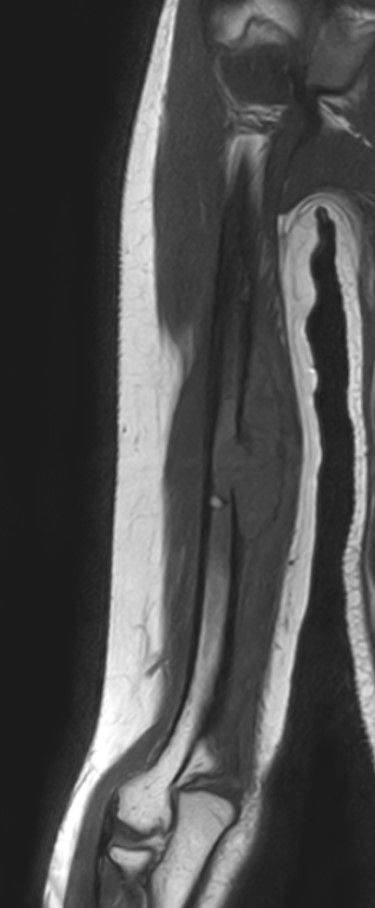
T2FS and T1 weighted coronal MRI images showing intramedullary lesion in mid diaphysis with cortical expansion and thinning with thin shell of bone and adjacent edema. Few cystic areas are also seen within the lesion. No fluid-fluid level seen
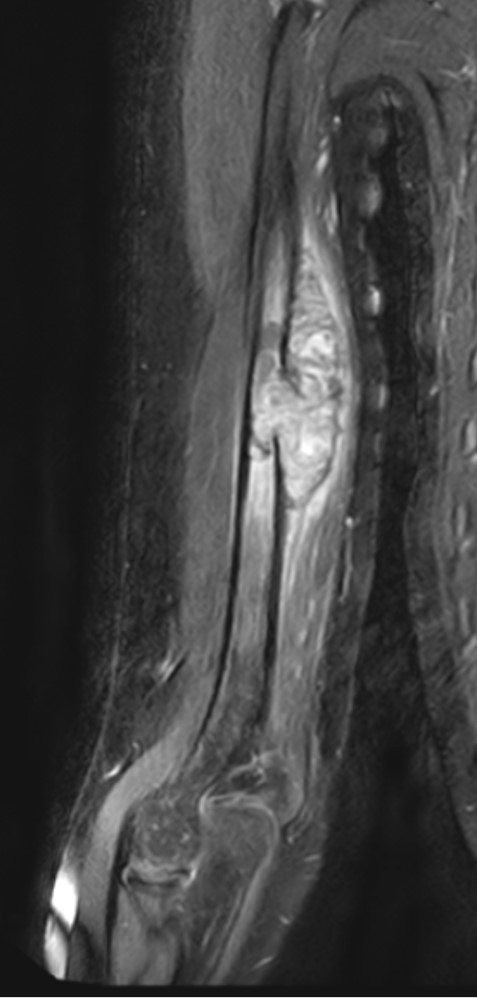
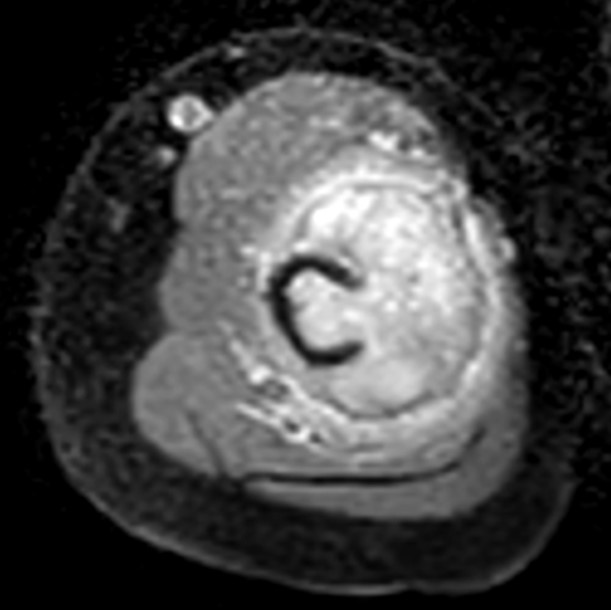
Heterogenous enhancement is seen on post contrast images

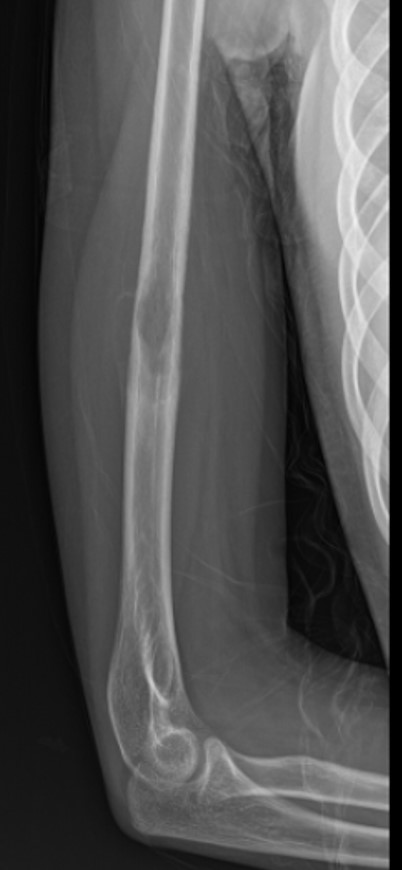
Radiograph done within a period of 4 months shows rapid increase in size of the lytic lesion with associated pathological fracture
Differential Diagnosis
| Telangiectatic osteosarcoma | Brown tumor | Aneurysmal bone cyst |
|---|---|---|
| Points in favour: • Rapid interval progression • Expansile lytic morphology • Enhancing solid component | Points in favour: • Expansile lytic lesion • Can show internal cystic change | Points in favour: • Marked bony expansion • Preserved thin rim of cortex • Absence of overt aggressive periosteal reaction or large soft-tissue mass |
| Points against: • No obvious cortical breach • No aggressive periosteal reaction • No large extraosseous soft-tissue mass • Relatively preserved thin cortical shell | Points against: • Solitary lesion • No other skeletal features of hyperparathyr–oidism • Normal serum calcium, phosphate, PTH. | Points against: • Diaphyseal location is relatively unusual • Lack of classic fluid–fluid levels on MRI • Presence of a prominent enhancing solid component |


Patient underwent wide local excision of the tumor
Final Diagnosis
Histopathological examination of the excised specimen revealed the diagnosis of
“Solid variant of Aneurysmal Bone Cyst”
Learning Points
- Rare bone lesion accounting for 3.4-7.5% of all ABC
- As opposed to classic ABC it is commonly meta-diaphyseal, however can occur anywhere, even juxta-articular
- It is not always expansile and does not always show fluid-fluid levels and imaging diagnosis is difficult in such cases.
- MRI shows predominant solid soft tissue component showing contrast enhancement.
- Accompanied by adjacent marrow and soft tissue edema
- Not all ABCs show classic fluid-fluid levels.
- Solid ABC is a great mimic and no location in a bone is an exempt
- Secondary solid ABC in pre-existing lesions, though rare, is known.
- Radio-pathological correlation is essential.
- Always exclude telangiectatic osteosarcoma.